

select search filters
briefings
roundups & rapid reactions
Fiona fox's blog
Speaking in the House of Commons, the Prime Minster has announced the plan for ‘living with COVID’.
Prof Ivo Vlaev, Professor of Behavioural Science, University of Warwick, said:
“In the new situation, there will be a mix of responses – some are likely to feel ready to drop restrictions that have been personally costly, while others will fear things are moving too quickly. Changing the rules will change behaviour, which often happens independent of attitudes – research so far has revealed all over the world that rules are the dominant driver of behaviour. So, without the rules, we usually see a gradual reduction and disappearance of protective behaviours, often irrespective of beliefs and attitudes. For example, there is continuous drop in the number of people adhering to advice to wear masks once it is no longer a rule despite people still saying it is a good idea.
“And once a certain tipping point is crossed, the social norm can flip, speeding up an overall change in behaviour. Having said that, our society does not behave as a homogenous group, because of differences in risks and circumstances faced by different groups; for example, clinically vulnerable because of age and health status (those will still avoid public places, while others such as young people will readily go back to their old-normal).
“The government needs to be crystal clear what behaviours were now recommended in order to avoid people left feeling uncertain about what behaviours were now ‘recommended’. In the new situation government cannot just say ‘be cautious’ because it is too vague – they must be as specific as possible (and also provide the resources some people need to comply).”
Julia Faulconbridge, the British Psychological Society’s Division of Clinical Psychology, said:
“We do have some concerns about the government’s decision to end the mandatory self-isolation period after a positive test due to the negative mental health impact this could have on those who are clinically vulnerable. Removing this, along with access to universal free rapid testing from 1 April, could increase worry and anxiety amongst the clinically vulnerable, and widen existing health inequalities amongst those whose friends, family and colleagues cannot afford to take tests before contact.
“For many who are clinically extremely vulnerable Covid still poses a serious health risk, so we need a plan from government that clearly sets out how we can protect those who will continue to be most at risk from Covid. We must protect against the most vulnerable in our society from feeling that they have no choice but to return to shielding, limiting their social contacts, interactions and living less full lives than those who are not clinically vulnerable.
“We are also concerned that the removal of all restrictions could have a disproportionate impact on those from lower socio-economic groups and other pre-determining factors which make them more vulnerable to catching Covid, such as ethnicity, age, mental illness and having a learning disability.
“Living with Covid does not mean consigning groups of our society to living in isolation, and it does not mean we have to put vulnerable people at risk of damage to their physical and mental health. Collective responsibility and coming together as society has been what has seen us through this pandemic so far, we must look to these values now and ensure no-one is left behind in the wish to declare the pandemic ‘over’.”
Dr Stephen Griffin, Associate Professor in the School of Medicine, University of Leeds, said:
“I am dumbfounded by the majority of these announcements. Some comfort can be taken from retaining an albeit whittled down ONS survey, but other than the note of caution evident from the CMO’s presentation yesterday, it would seem that the over reliance on an as yet incomplete vaccination programme is the sole remaining protective measure left for the UK population.
“The announcement of further boosters for vulnerable groups is welcome, but this is only necessary because of the unrelenting prevalence of virus infection resulting from a complete lack of control.
“Moreover, the over reliance on vaccination is a stark contrast to the lacklustre announcement of 5-11 year olds being able to access this now essential stand alone protection. I would urge that this is brought forward ASAP.
“The simple fact is that vulnerable people are once again being ignored as the government discards what it terms “restrictions to our freedom”, when these are in fact liberating for those who remain at increased risk.
“Vulnerable people require others to test, wear masks and isolate in order to prevent their exposure to infection. These trivial, and now familiar exercises are a small price to pay in order to allow everyone to move forward together.
“Another theme from yesterday was the opportunity to pay for testing, and advice to isolate when symptomatic but without financial or legal support. This exacerbates inequalities already present in society, and I would suggest that the vast majority of families can ill afford sufficient LFDs to act responsibly.
“Yes, testing is expensive, but has this been balanced against economic gains from ensuring safe working? The irony of the government complaining about expenditure after the shameless exploits around PPE contracts and the private contracts used for the contact tracing programme is tangible.
“Much was made yesterday about excess deaths and the reduced severity of omicron compared to other VoC. Yes, there is a reduced case fatality rate (cfr), for omicron compared to delta, but the risk of hospitalisation remains and is equivalent to Delta for under 18s according to the imperial study. Moreover, the clinical impact is proportionate to both the cfr and the number of infections, a strain being borne yet again by our underfunded and understaffed NHS.
“The notion that the omicron wave has resulted in fewer deaths than expected is undermined by the inclusion of 2021 as part of the 5 year baseline for excess deaths. I am not a biostatistician, but including a pandemic year as a benchmark must scream out at even the most mathematically challenged amongst us. Why was this necessary? Whilst fewer people have required treatment in ICU, hospitalisations remain high as do deaths, considering what might otherwise be achieved if our vaccines were used sensibly alongside other measures.
“These plans make no provision against long COVID. Although it is now clear that vaccines give protection, breakthrough and reinfection, even with few symptoms, can lead to long term health problems. The lack of protections in schools is also increasing the number of children self-reporting such problems, which is a tragedy.
“Naturally as a virologist I am also concerned that allowing high prevalence in a partially vaccinated population is a recipe for virus evolution to accelerate, and as the CMO and CSO said, we cannot predict the origin or nature of the next, inevitable VoC. Standing down our safeguards under these circumstances feels speculative at best, and could undermine any hope of a preemptive rapid response to a new wave of infection.
“Lastly, it should be recognised that we appear to be moving towards a “focused protection” model of pandemic control, such as advocated by the Great Barrington declaration in the past. Now, boosters and antivirals have replaced isolating millions of people, but the flaws in this approach remain. Practically, it is impossible to conclusively define those in need, or who are likely to need protection in the future. However, from an ethical and moral standpoint, I would suggest that we remember Ghandi’s words, and not disregard those least able to help themselves, whether they are vulnerable for health or socioeconomic reasons.
“These actions will inevitably prolong, rather than curtail the pandemic. Living with something is not the same as ignoring it.”
Dr Raghib Ali, Senior Clinical Research Associate, MRC Epidemiology Unit, University of Cambridge, said:
“As infections, hospitalisations and deaths are currently falling and based on previous experience of when restrictions have been lifted (e.g. when Plan B ended and on July 19th) it is unlikely that moving from mandates to guidance on self-isolation will lead to a significant increase in infections, hospitalisations and deaths.
“This is partly due to the extremely high levels of population immunity we now have, with over 98% of adults having antibodies, and over 95% of the over 60s having had boosters.
“But also because the majority of people will continue to self-isolate – as we have seen with most people continuing to wear masks and have reduced contacts even after there was no legal mandate. As we saw during the most recent omicron wave voluntary changes in behaviour produced the same outcome as expected with a return to step two of the roadmap – and so it is clear that people can be trusted to take personal responsibility for their actions – based on the level of risk at the time – without government mandates.
“Also, with any restrictions, levels of compliance are also critical to their effectiveness. For example, household mixing (a key route of transmission) has been shown to have fallen between lockdowns when cases were rising – but mixing was allowed – and risen during lockdown 3 when cases were falling and the vulnerable had been vaccinated – even though it was illegal. i.e. mixing was more influenced by the level of risk (cases rising or falling) than the rules in place at the time.
“I welcome the clear guidance from the CMO/NHS that people should continue to self-isolate when symptomatic or testing positive while prevalence of infection remains high.
“I also welcome the continuation of the ONS infection survey and genomic surveillance to ensure that we are well prepared for whenever the next variant inevitably arrives.
“I think it would be better to continue current levels of sick pay while prevalence of infection remains high to discourage ‘presenteeism’ for those who are unable to work from home.
“We also need to reassure those who are most vulnerable to Covid that these changes are unlikely to significantly increase their risk and they should be given clear guidance that well-fitted FFP2/3 masks do provide them with good protection (as they have for frontline NHS staff).
“With regards to free testing, I agree that we should continue providing limited free tests (some people are over-using them) until April 1st and if prevalence remains high, I think they should be continue to be provided to those who would be unable to afford them.
“It is also important to remember that as prevalence falls, the relative benefit of mass testing decreases – i.e. the number needed to test to prevent one infection/admission/death increases and so the cost/QALY gained increases – and mass testing (as well as other nonpharmaceutical interventions) should be subject to the same criteria as any other intervention – i.e. Do they have a clinically significant benefit? Does that benefit outweigh any harms? And are they the best use of resources – or would spending money on something else produce greater health benefits?
“And so I think it is essential to initiate randomized-controlled trials of mass testing (as well as other nonpharmaceutical interventions) to assess their effectiveness in actually reducing infections, admissions and deaths in a highly immune population so we have better evidence before the next variant arrives.
“Finally, although we are in a much better position now, COVID is not over and we should continue to use our freedoms responsibly to protect those at highest risk.”
Professor Dame Anne Johnson PMedSci, President of the Academy of Medical Sciences, said:
“Only time will tell if this is the right moment to drop all restrictions and we will need more details to fully understand the Government’s plan.
“The Office for National Statistics Covid Infection Survey and the surveillance coordinated by the UK Health Security Agency have been powerful tools in monitoring the spread and variants of COVID-19, so it is to be welcomed that these essential systems are being prioritised. However, we need to understand the extent to which they will be scaled down, and the scientific basis for ensuring that they will be fit for purpose to detect trends and new variants.
“Despite the changes being made, we all still have a collective responsibility to keep protecting the people who are at greatest risk from COVID-19. Although it will no longer be a legal requirement to self-isolate [from Thursday 24 February], people should continue to take precautions and modify their behaviour to reduce spreading the virus especially to those who are vulnerable. This includes getting COVID-19 vaccinations and boosters and people staying at home when they are ill where possible. These are vital steps to protect our most vulnerable members of society. The pandemic has already disproportionately impacted more disadvantaged communities and the removal of financial support for self-isolation means that many will not be able to afford to self-isolate.
“While maintaining the current level of testing is not sustainable in the long-term, we need a better understanding of how symptomatic testing will be prioritised in future based on clinical need so that those who need it can get a diagnosis, access care and receive appropriate treatment.
“When infection rates are high, testing must also continue to be available to protect those who are at high risk of severe disease (and the people around them) and in high-risk environments such as in healthcare settings and care homes, and clarity is needed on how this will continue. Testing is also vital for potentially life-saving research, such as the UK’s PANORAMIC trial looking into new antivirals.
“As ever in any crucial stage of the pandemic there are no perfect solutions, but clear communication is key and we look forward to the further clarification as promised in the plan.”
Prof Penny Ward, Independent Pharmaceutical Physician, and Visiting Professor in Pharmaceutical Medicine at King’s College London, said:
“Based on the reaction of some, one might think that we are going from total restrictions to total freedom in one bound but actually todays message is one of a staged winding down of various measures as the outbreak steadily wanes hopefully to disappear more completely as spring arrives. One would hope by this stage in the pandemic, the general public would be well aware of the need to self isolate if infected with covid to prevent transmission of infection to others. Certainly the behaviour of the public after relaxation of Plan B measures suggests that they are quite likely to act responsibly in future. Of course, removing the legal requirement to isolate also removes access to the isolation payment. Individuals in jobs which cannot be done remotely may force some onto SSP, which does not kick in for 4-7 days, making life difficult for the lower paid. Given the difficulty finding workers currently, perhaps some employers will step into the breach and support their workforce to enable self isolation when needed without fear of financial difficulty. Access to free testing continues for the time being but with a plan to phase this out from April. Enhanced surveillance will continue to detect outbreaks and new variant emergence throughout the year. Access to free tests will continue for some occupations and for some individuals, but the details are not yet decided. Again, some employers may elect to continue to provide testing services for their employees, particularly those seeking to encourage people to return to office environments. The CMO and CSO this evening were at pains to point out that the NHS would continue to test those needing to be tested to enable appropriate management – perhaps ahead of planned surgery or other hospital treatment as well as to enable rapid diagnosis of covid in those eligible for antiviral treatment. For those of us neither in work nor in an antiviral eligible group, there will still be access to testing if we are willing to pay, as is currently the case for tests needed for travel. Perhaps an increase in the numbers paying for testing might bring down the price to a more manageable level – we live in hope!”
Dr Freya Jephcott, Senior Research Associate the University of Cambridge, and convener of the Hidden Epidemics and Epidemiological Obfuscation Research Network, said:
“Free and ready access to testing should be at the heart of our strategy for living with COVID-19. To roll back testing at this moment will severely impair people’s ability to care for themselves and protect those around them. It will also lessen our ability to mitigate the fallout from future waves of infection.”
Prof Trish Greenhalgh FMedSci, Professor of Primary Care Health Services, University of Oxford, said:
“Today’s announcement is not a plan for living with Covid, it is a plan for reducing spending on testing and cutting support for people who have or may have Covid. Learning to live with Covid does not mean pretending it isn’t highly prevalent or pretending the virus is no longer dangerous. Learning to live with Covid means having a clear plan for preventing its spread and protecting those at risk of poor outcome. Vaccination is important, but it will not contain the virus if it is used as a sole measure. We need a ‘vaccines-plus’ strategy, comprising 1. Unequivocally declare Covid-19 to be an airborne disease and plan preventive strategies accordingly; 2. Until the prevalence has fallen substantially, require high-quality masks in all indoor spaces and especially on public transport; 3. Improve and monitor air quality in public buildings; 4. Set criteria for introducing/relaxing measures as case numbers rise/fall; 5. Support those who need to isolate; and 6. Strive for global vaccine equity, since an undervaccinated global population is inequitable and also brings a risk to everyone.”
Prof Christina Pagel, Professor of Operational Research, UCL, said:
“The long term future for the ONS National Infection Survey is welcome and crucial in underpinning any response to future variants and waning vaccines. However, removing free testing more generally has many disadvantages. Firstly, the Prime Minister spoke about “individual responsibility” but access to tests in one of the key ways we can exercise responsibility. Without it, it will be harder to know you are infected and to behave accordingly; it will be harder to know if rates are high in your neighbourhood and so whether you feel comfortable meeting others in public spaces, or going shopping without a mask for instance. While the government is offering a fourth dose to the most vulnerable, data from Israel showed that this had limited impact against Omicron and we do not know how effective it will be against future variants as the virus evolves further and further away from its original form (which the vaccines are based on). Particularly the clinically extremely vulnerable, therefore, will be forced into living a permanently more risky life or a less full one.
“Removing self isolation requirements, financial support for self-isolation and free testing will disproportionately affect more deprived communities. People within those communities will be less able to afford testing, less able to afford to isolate and more likely to work outside the home and so potentially infect others. Combined with higher rates of existing health conditions and lower rates of vaccination, this is likely to lead to significantly higher burden of covid and its consequences in these communities compared to the least deprived. Where are the plans to tackle health inequalities, to improve sick pay, to improve workplaces and spaces to have cleaner air?
“If we are to add a new, serious, disease that is far more infectious than flu to our population with no adaptations to indoor environments or way of life then we must expect frequent reinfections, more ill health and many more deaths each year. There is nothing particularly normal about reversing decades of progress in drastically reducing the impact of infectious diseases and improving public health with barely a whimper.”
Prof Mark Woolhouse, Professor of Infectious Disease Epidemiology, University of Edinburgh, said:
“I agree with the UK government that the trends in the Covid-19 data – particularly the steady fall in hospitalisations – support the further lifting of restrictions at this time. However, there is a legitimate concern that taking this step could lead to a resurgence in cases.
“As always, what the government does or does not ask of us is much less important than what we actually do. Throughout this pandemic the public have consistently been prepared to change their behaviour not just in response to rules and regulations but also in response to their own perception of the risk to themselves and others.
“The idea that people would immediately return to pre-pandemic behaviour patterns when restrictions were relaxed was one of the main reasons why the models have twice been much too pessimistic; first when many restrictions were lifted back in July 2021 and again when the omicron wave hit in December. In practice, people have been much more cautious and responsible than many experts predicted.
“If that pattern is repeated – encouraged by robust public health advice and enabled by access to testing and support for those off work – then I don’t expect this latest round of relaxations to have a dramatic impact on the short-term course of the epidemic.
“The most likely problem in the medium term is the (almost inevitable) appearance of another variant. It is important that the public health agencies across the UK have plans in place to respond to that rapidly (within days) when it happens. If those plans include measures such as the rapid roll-out of self-testing kits – which worked extremely well during the omicron wave – then it is vital that the infrastructure is in place to deliver that very quickly indeed.”
Prof Rowland Kao, the Sir Timothy O’Shea Professor of Veterinary Epidemiology and Data Science, University of Edinburgh, said:
“The critical concern here is the evidence that, while by most metrics COVID-19 is largely in retreat or at least relatively stable across in the UK, this is occurring unevenly. The evidence suggests that deprivation remains an important factor in the relative stress that COVID-19 is putting on local communities. For example, ICU occupancy and deaths are now increasingly due to people living in the most deprived areas. This is likely partially due to vaccination patterns, with uptake in deprived areas lower than in more affluent ones. The lower uptake will be due to many factors, including age distributions – with younger men in particular still less likely to get vaccinated. Whatever the cause, it does mean that more virus is likely to be circulating in those deprived areas. Also, vaccination alone doesn’t fully explain the observed patterns, as the distribution of lateral flow tests is also uneven – fewer tests taken and higher proportion of positive tests in deprived areas.
“As the requirements to isolate are released (and therefore with no compensation for isolating) and with the expectation that free testing will also be removed, this will likely most impact those who are under the most pressure to work in places where distancing is difficult and therefore potential exposure to infection high. They are also individuals most likely to be under financial pressure to continue working if able. They are also people in the areas which, because of existing health deprivation, are most likely to have severe outcomes. We do not of course know how severe such challenges will be – we shall only know as we go forward and here, changes in data streams also means it will be increasingly hard to monitor the impact of changes, until changes in the most severe outcomes (hospitalisations, ICU occupancy and mortality) are apparent. However, while it is acknowledged that continued restrictions such as we have now are unsustainable in the long term, releasing all restrictions so quickly does represent a gamble and one that, if it fails, will likely have the most impact on those who are already disadvantaged.”
Prof John Drury, Professor of Social Psychology, University of Sussex, said:
“Policy changes, including dropping of measures, have a strong signalling effect, informing public judgements about seriousness and risk – as has been shown at several points during the pandemic including so-called ‘freedom day’. Therefore, likely impacts of the government announcement’s that the legal requirement to self-isolate is to be dropped from Thursday will include significantly reduced perceptions of risk among the public and so fewer people self-isolating. Given that financial support (or lack of it) is a major driver of adherence to self-isolation, dropping the £500 compensation for self-isolation provided to a minority of people will reduce risk perceptions, reduce self-isolation, and likely lead to a spread of infection disproportionately amongst less privileged groups.”
Comments sent out 20/02/2022 – 21/02/2022 on the forthcoming ‘living with COVID’ plan, before Boris Johnson’s statement to the House of Commons:
Prof Sheila Bird, Formerly Programme Leader, MRC Biostatistics Unit, University of Cambridge, said:
“Lateral flow device (LFD) antigen tests have not been free. They have been paid for by thee and me, out of the public purse. But we have not had choice about which 7-pack of LFDs has been issued to us.
“Before the government opens up the LFD-market to citizens’ choice, the government and Medicines and Healthcare products Regulatory Authority (MHRA) need to put into the public domain all dual-testing evidence held per LFD-type about its sensitivity for asymptomatic testing; or explain why such data are lacking – particularly given the role of Department of Health and Social Care as “LFD-manufacturer”.
“Below, I summarise some [by no means all] of the PCR and LFD data reported by NHS Test and Trace during the peak of the Alpha and Omicron winter waves of the SARS-CoV-2 pandemic. Notably absent from management information published by NHS Test and Trace are cycle-threshold values for PCR-positives & LFD-type.
“Even retrospectively, during rising winter waves of SARS-CoV-2, Tables 1 & 2 reveal just how tricky it is to interpret different testing-routes (by test-type) when access to them and tolerance for them have changed markedly over time. Robust, well-designed-and-analysed, well-accepted, cost-efficient SAR-CoV-2 PCR plus ct-threshold plus genomic surveillance remains essential going forward.
“For details, please see Table 1 and notice that:
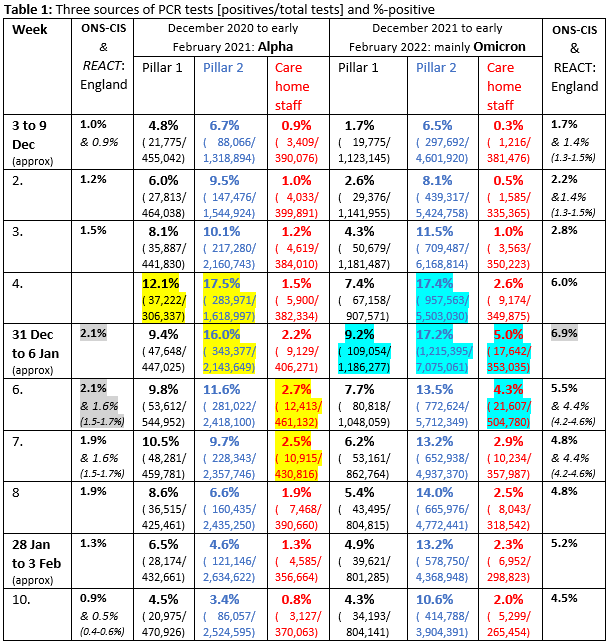
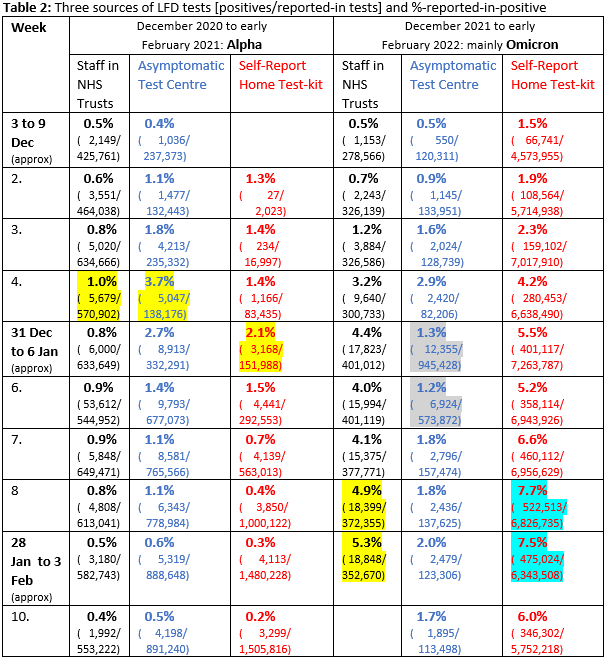
“Moreover, Table 2 reveals the following about reported-in LFDs (LFD-type not in public domain):
“Even retrospectively, during two winter waves of SARS-CoV-2, Tables 1 & 2 reveal just how tricky it is to interpret different testing-routes (by test-type) when access to them and tolerance for them have changed markedly over time. Robust, well-designed-and-analysed, well-accepted, cost-efficient SAR-CoV-2 PCR plus ct-threshold plus genomic surveillance remains essential going forward.”
Dr Simon Williams, Lecturer in Psychology, Swansea University, said:
“It is expected that the legal requirement to self-isolate will be being axed as part of a forthcoming “living with COVID” strategy. I, like many in public health and healthcare1, feel that it is too early to remove this protection.
“One reason why it is too early is because we don’t know how people are going to behave in the absence of this legislation – we don’t know how many people are going to voluntarily self-isolate if they feel unwell with symptoms which may be related to Covid. Our behaviours, like the virus itself, can be hard to predict for scientists.
“Although we know adherence to COVID-19 measures has been, on balance, very high2 throughout the pandemic, research has begun to emerge3 which suggests that some form of ‘pandemic fatigue’ does eventually set in, particularly for ‘high-cost’ behaviours such as lockdowns4, restrictions on visiting others5. Self-isolation is a ‘high cost’ behaviour; it’s hard.
“We shouldn’t assume things will completely return to a pre-pandemic ‘normal’, where people generally weren’t self-isolating as a precaution to avoid passing on a virus but were ‘soldiering on’ and staying at home only if they felt too unwell to go to work for example. The pandemic has changed our behaviour – after two years, many of us are still avoiding some of those everyday behaviours6 like hugging or shaking hands with people outside our household. Moreover, nearly three-quarters support keeping the legal-requirement to self-isolate according to a recent poll7, suggesting that many feel self-isolation is still important.
“However, it is reasonable to expect that removing rules will likely lead to a decrease in a behaviour, including self-isolation. We see this with mask wearing. Data8 shows how mask wearing dropped off in England last summer following the removal of the requirement to wear them in some indoor settings. Over the past few weeks, we are again starting to see sharp drops in mask wearing in both England and Wales (despite Wales still requiring them in some settings), in people of all ages. This is despite mask wearing being a relatively ‘low’ cost, habituating behaviour9.
“One thing we can be confident in is that most people don’t necessarily lack the motivation to self-isolate, but some definitely lack the financial and practical support to be able to do so. Choosing between staying at home when sick to protect others and losing income is a choice no one should have to make.
“And so, governments will have to make sure that workers and employers are encouraged and supported to be able to self-isolate. Ensuring that statutory sick pay is sufficient, and continuing to make it available from day one would be a good start. We also need to continue the cultural change around presenteeism – employers and organisations need to encourage and enable workers to work from home or stay at home (depending on circumstance and job type) when unwell, and so supporting continuing hybrid working arrangements will help many to stay or work at home, if unwell.
“We also need to rethink keeping free lateral flow tests. With testing, reducing people’s opportunities and capabilities10 to test easily, will lead to a reduction in the behaviour. Earlier in the pandemic adherence to lateral flow testing was low11, but this was higher this past winter12, as free testing was accompanied by a clear message over its usefulness. Having to pay for free tests will disproportionately affect those on the lowest incomes, who, because of the lower vaccination uptake13 within their communities and because their jobs are often higher-contact14, have been most affected15 by Covid.
“After two long years, we have a lot to be optimistic about. Some mobility data16 suggests we are already back to pre-pandemic levels of mobility. We don’t want to throw the baby out with the bath water, and self-isolation remains an important way to protect ourselves and others, as we as we continue, cautiously, to put the past two years behind us and get on with our lives.”
1 https://www.nhsconfed.org/publications/cautious-exit-leaders-views-living-COVID19
2 https://www.covidsocialstudy.org/
3 https://www.nature.com/articles/s41562-021-01181-x
4 https://www.nature.com/articles/s41598-021-02133-1
5 https://www.nature.com/articles/s41598-021-02092-7
8 https://cmmid.github.io/topics/covid19/reports/comix/Comix%20Weekly%20Report%2098.pdf
9 https://www.nature.com/articles/s41562-021-01181-x
11 https://bmjopen.bmj.com/content/12/2/e058060
16 https://covid19.apple.com/mobility
Dr Simon Clarke, Associate Professor in Cellular Microbiology, University of Reading, said:
“The government’s move towards abandoning compulsory isolation might be politically brave, but it could end up exposing a lack of defences against even this wave, let alone any new more dangerous variants. As NERVTAG recently pointed out, it is a “common misconception” that the virus will definitely become less lethal over time, nobody knows what the Covid-19 weather has in store for us.
“This is not a move motivated by data, despite what ministers will doubtless say; they have never outlined what the national Covid-19 picture would need to look like for this to happen. Instead, they will expect people to swallow assurances that this is what the government were waiting for all along. Comment and insight from the Chief Medical Officer or Chief Scientific Advisor are notable by their absence. It seems to be a government pantomime geared towards persuading people that it’s all over and I expect that in the coming days it will be linked to helping the NHS get back on its feet. However, allowing infections to run riot in the community and be transferred into hospitals, which they will probably end up being unfairly blamed for again, will just cause more problems in vulnerable patients.
“A shift away from a legal obligation to isolate with symptoms or a positive test, and towards personal responsibility and choice, will put their onus on individuals, employers, and institutions such as hospitals and care homes to interpret the latest guidance and impose their own rules. This could lead to such a complex mix of guidelines and regulations that many people struggle to interpret them. It has been hard enough encouraging people to stay at home when sick even with national guidelines and systems of government support.
“The Queen’s situation also reminds us of what is at stake as the rules on isolation and other restrictions set to change in the UK next week. The news that Her Majesty has covid will no doubt be of great concern to her family and the whole country. While reports from the Palace that her symptoms are mild are encouraging, we must remember that at 95, the Queen is in the age group that is most vulnerable to serious disease and hospitalisation. Those over 85 are more than 300 times more likely to die from a covid infection than a young adult under 30. However, we know that vaccines play a major role in keeping symptoms milder in all age groups. Assuming the Queen has been infected with Omicron, the current dominant strain in the UK, we should remember that while omicron seems to cause fewer people to be seriously ill than previous variants, it can and does still kill people. We know that having had three jabs makes anyone much less likely to be seriously ill or die when infected with covid. It could be that the difference between the reigning monarch in the United Kingdom being a Queen or a King this week are three regular doses of Covid-19 vaccine.”
Prof Lawrence Young, Professor of Molecular Oncology, University of Warwick, said:
“If the legal requirement for self-isolation is removed and if the testing regime is to be dismantled, in the face of high levels of infection, this would inevitably increase the spread of the virus. Learning to live with covid doesn’t mean ignoring the virus and hoping it will go away. We need to learn to live safely with covid and that means retaining basic surveillance as well as case isolation.
“With 1 in 20 people in England infected with the virus and around a third of the population not having had a booster vaccine dose, now is not the time be abandoning measures that will keep us all safe. As long as the virus continues to spread and replicate, particularly in populations who are under-vaccinated, it will throw up new variants and these will remain a continual threat even to those countries with high rates of vaccination. It would be wrong to assume that any new variant will be less infectious and less dangerous particularly as vaccine-induced immunity wanes and may not be as protective against these new variants.
“We need to find a new normal where we maximise our freedoms while recognising that covid will always be present rather than trying to return to a pre-pandemic world where covid doesn’t exist. This requires clear messaging from government about the need to remain vigilant and to take personal responsibility in protecting family, friends and work colleagues from infection. We need to maintain our test and trace capacity and do everything to protect those who are most vulnerable. You can’t control virus infection if you don’t know where the virus is and how it is spreading. This means planning for future surges of infection by ensuring we have the ability to rapidly detect outbreaks with targeted approaches to test, trace and isolate. Key to this is maintaining free access to lateral flow tests for all those with symptoms and maintaining the ONS Infection survey as a way of monitoring community infection and the arrival and spread of new variants. The pandemic isn’t over and, if we’ve learnt anything over the last 2 years, it’s that the impact and future course of covid-19 is unpredictable. This is not the time to let our guard down.”
Prof Robert Dingwall, Professor of Sociology, Nottingham Trent University, said:
“It is clear that many natural scientists, and some behavioural scientists, are very naive about the impact of laws and regulations, and why there is little value in retaining them. They are not like the supposed laws of physics.
“The field of socio-legal studies has not been drawn into the design of pandemic management. However, it has long been recognized that laws are not self-interpreting or self-enforcing. There is now emerging evidence from socio-legal research about the extent of ‘creative compliance’, where people interpret pandemic rules flexibly to suit their own circumstances, as they do in almost every other sphere of life. If they are sanctioned for this, they, and others around them, are likely to feel unjustly treated. They lose confidence in the fairness of the law and those who make it. Enforcement agencies lose the trust of communities, which may be important to them in other ways. By now, these agencies have largely abandoned any attempt to make pandemic rules stick, even under pressure from health departments.
“In legal terms, pandemic management has been a mess from the very beginning, confusing citizens with the frequency of changes and the randomness of enforcement. It has never met basic requirements of the rule of law. I suspect that few of us who have spent much of our careers studying the interactions between law and society will be sorry to see the legislation go. It has become pure theatre, standing in the way of a ‘soft landing’ and a gradual transition to a stable relationship between virus and society.
“Socio-legal change of this kind is not a cliff edge, as we saw with Freedom Day last summer. Large numbers of people are not going to start changing their behaviour overnight – but behaviour will gradually shift, as it did last year. Creative compliance will come out of the shadows as people decide what precautionary measures suit their own lives, circumstances and tolerance of risk.
“Over the next few months, we should expect to see an accommodation emerge between the population and the Covid virus, much as we have with every other respiratory infection. This process will only be disrupted if particularly risk-averse public bodies try to hold back the tide by looking for legal loopholes, like conditions of carriage on transport systems, that allow them to continue restrictions. The equilibrium may not be in a place that everyone likes but that is how democracy works.
“The next challenge is to learn from the failures of law and regulation that resulted from rapid and sloppy drafting and ill-considered sanctions. Public health and civil emergency legislation clearly require thoughtful modernization before they are ever invoked again. This work needs to be based on socio-legal research about the actual operation and impact of laws and regulations rather than the assumptions or suppositions of the biomedical or behavioural sciences.”
Prof Susan Michie, Director of UCL Centre for Behaviour Change, UCL, said:
What do we know from evidence about how seriously people take public responsibility versus abiding by laws? Do we know from evidence whether the public has responded only to the law during the pandemic or whether they have also changed their behaviour due to their own feelings about the situation and the state of the pandemic and/or to public health advice?
“Throughout this pandemic, people have generally shown support for Covid19 public health measures, often adopting them before Government legislation for them. Public opinion surveys have shown that there is generally significantly more support for retaining rather than dropping such measures.
“Legislation for a Covid19 public health measure communicates two things: that not complying will result in a financial penalty and that the measure is sufficiently important to underpin it with legislation. We know from changes in legislation for facemasks in England that use sequentially increased, decreased, increased and then decreased according to whether there was legislation in place.
“The Corsair study’s analysis of 64 cross-sectional surveys between February 2020 and January 2022 (n≈2,000 per wave) found that over two years, people have continued to adopt personal protective behaviours intended to prevent the spread of COVID-19. However, it also found that the greatest variations in behaviour reflected changes to Government rules, with out of home activity mirroring the easing and re-introduction of rules.
“An important influence on behaviour is the desire to fit in with social norms, that is to behave in line with what’s seen as normal, acceptable or respectful. Given most people obey the law, majority adoption has the effect of further influencing those who don’t want to be seen as different. Removing legislation is likely to result in minority adoption, which will then have the opposite normative influence, making the minority feel different and therefore less likely to, for example, wear facemasks. It is also likely to increase tensions between those who continue to adopt the behaviour and those who do not.
“Isolating from others when likely to be infectious is a more complex behaviour than wearing facemasks as it depends on a conjunction of practical as well as social factors, for example, being able to afford to stay at home and to hand over outside responsibilities, and having managerial and peer support for not going to work. Pre Covid19, there was a well-documented problem of ‘presenteeism’ at work, with people going to work with infectious illnesses such as coughs and colds: indeed, this was often perceived as commitment to the job and helping out peers rather than as an antisocial act. With the potentially serious short-term effects of Covid19, and unknown long-term damage of long Covid, it behoves Government and employers to end the culture of presenteeism and do everything possible to support those who may be infectious to stay off work and at home.
“A recent statement from SAGE’s behavioural group (SPI-B) stated “If the legal requirement to self-isolate upon testing positive is lifted and becomes an item of public health guidance, it is likely to lead to further ambiguity among the public about the need for strict adherence. This will disproportionately impact vulnerable sections of the population, for example those who face greater pressure to work outside the home when ill because of financial hardship, precarious employment, or caring responsibilities… Other countries’ efforts to reduce rates of infectious illness through improved sick pay have proved effective. There is scope to trial this in the UK and other ways to help people to stay at home when infectious.” (https://www.gov.uk/government/publications/spi-b-social-and-behavioural-impacts-for-lifting-remaining-restrictions-10-february-2022).”
Dr Michael Head, Senior Research Fellow in Global Health, University of Southampton, said:
“The UK government response has overall been typified by a ‘too little, too late’ or ‘too much, too soon’ agenda. For example, too late to put interventions in place, or too soon with lifting those restrictions, when just a few weeks more would be eminently more sensible. Here, we have the latest in a long line of reckless policies.
“As reported by the government dashboard, there are still hundreds of COVID-19 deaths a week, with tens of thousands of new cases every day, and over 1000 people being admitted with covid19 to hospital every day. There appears to be little to no consideration of vulnerable populations, who either cannot be vaccinated or generate a reduced immune response to the COVID-19 vaccines. There are still millions of people who need their booster dose. Children aged 5-11 years, who have rather been the punchbag population throughout the pandemic, also need to be vaccinated, to protect them as individuals and those around them.
“It appears that healthcare workers, including those in social care, will still have access to free tests. Assuming that is the case, this is the correct move. There does not appear to be a firm decision yet about whether the rest of the population will be charged to take a lateral flow test, though recent comments appear to indicate that is to some extent current thinking. In the short-term, it would be a ridiculous move – few people will take tests if they have to pay, and thus surveillance will suffer. The surveillance must be bolstered by continuation of the ONS surveys, since this will be our most reliable way of measuring prevalence in the population. This will contribute to our early warning system against any waning of immunity and future spikes in new cases. If we were to bring COVID-19 cases down to genuinely low levels, then the availability of free tests would still be of public health benefit, and therefore not expensive for the government budgets.
“Keeping some measures in place, including for example the requirement to wear masks in indoor spaces and requirements to self-isolate, for a few more weeks would be helpful. Breaking chains of transmission means there would be fewer people unwell and in hospital, healthcare resources would be freer to address their extensive backlogs, and more people would have received their booster doses thus ensuring they are better protected.
“Supporting people to stay at home when they test positive is vital, especially since we have seen greater burdens of disease in those who work in lower-paid employment and can less afford to take time off work.
“There are so many reasons why low levels of covid19 are good for the population, including patient care in other areas of health, the economy, and our mental health and wellbeing. A little caution goes a long way. Why is the government so consistently reckless with the health and wellbeing of this country?”
All our previous output on this subject can be seen at this weblink:
www.sciencemediacentre.org/tag/covid-19
Declared interests
Dr Stephen Griffin: “Member of Independent SAGE.”
Prof Mark Woolhouse: Author of ‘The Year the World Went Mad: A Scientific Memoir’ about the pandemic.
Prof Sheila Bird: “Member both of RSS COVID-19 Taskforce and RSS Working Group in Diagnostic Tests; also member of UKHSA’s Testing Initiatives Evaluation Board. SMB posts in a personal capacity.”
None others received.