

select search filters
briefings
roundups & rapid reactions
Fiona fox's blog
The Office for National Statistics (ONS), have released the latest data from their COVID-19 Infection Survey.
Prof Sheila Bird, Formerly Programme Leader, MRC Biostatistics Unit, University of Cambridge, said:
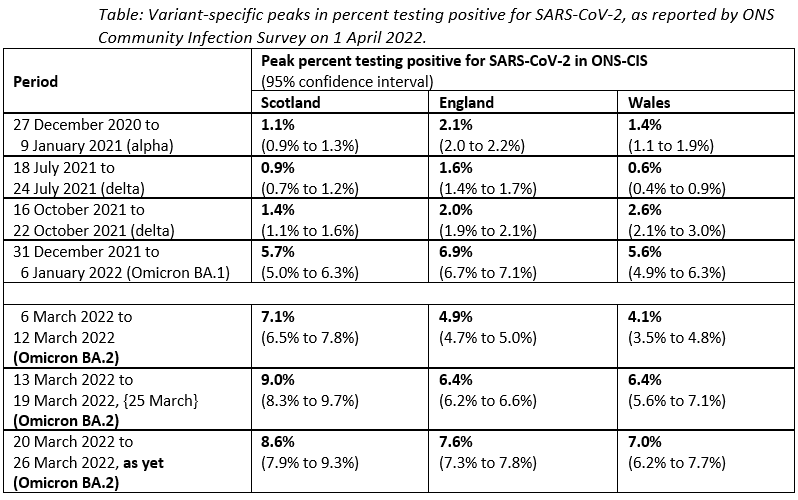
“Today’s release by ONS Community Infection Survey confirms that, for whatever reason and unlike for previous variants, Omicron BA.2 has hit harder (by 40% @ 25 March) and earlier in Scotland (by 2 weeks) when compared with a) Omicron BA.1 in Scotland or b) Omicron BA.2 in England & Wales, see last three lines of Table.
“The implication for COVID-mention deaths by occurrence-week is that England’s Omicron BA.2 peak will be 2-weeks later than in Scotland (where Omicron BA.2 peak is already 50% greater than for omicron BA.1) and may be as concerning pro-rata unless the 4th COVID-vaccine intervenes to England’s advantage.”
Dr Julian Tang, Honorary Associate Professor/Clinical Virologist, Respiratory Sciences, University of Leicester, said:
“Although the COVID-19 case numbers and hospitalisations and deaths in those with COVID-19 are indeed rising, we now need to see this in the specific context of learning to live with COVID-19.
“In a well-vaccinated population (though the vaccine is now 2 years old and was designed against the original Wuhan virus), mitigating against more severe disease and death, the comparison with seasonal flu – including the degree to which we accept a certain amount of COVID-19-related morbidity and mortality – is now more relevant.
“A zero COVID approach is and has really never been possible in the UK, where people highly value their individual freedoms and social liberties. So now, we need to balance the amount of COVID-19 related healthcare impact against other demands on the healthcare system and other aspects of society.
“Ideally, I would have preferred to see a more tapered approach to the removal of COVID restrictions – perhaps keeping the mask mandate for longer, as well as maintaining free testing and more of the COVID-19 surveillance/survey programmes – to spread this omicron surge over a longer time period. But we don’t do any of this for seasonal flu – and we live with whatever it throws at us each year. If we applied the same non-pharmaceutical restrictions to seasonal flu as we do for COVID-19, we would also see a reduction in seasonal flu morbidity and mortality – but this will also come at some cost to social and mental health and the economy.
“Eventually, COVID-19 will become more endemic and seasonal – like flu (which also generates many new circulating variants) – and I suspect that we will end up dealing with it in the same way each year: with focused vaccination/booster programmes for those most vulnerable – perhaps including school children to reduce the seasonal spread of the virus (as we do with flu in the school vaccination programme) – and a pared down national surveillance programme using sentinel sampling sites (GP clinics and hospitals), with ready dispensing of antivirals (e.g. paxlovid, molnupiravir) that can be taken at home to mitigate against severe disease – as we do each season with flu (with oseltamivir).
“Then beyond this, we will deal with seasonal surges in COVID-19-related hospital admissions as the virus will exacerbate other chronic conditions, like diabetes, chronic heart, lung, kidney and neurological disease – as we do with seasonal flu each year.
“Finally, I don’t think the statistics separating hospitalisations with COVID-19 and for COVID-19 are necessarily very helpful, as COVID-19, like flu, can exacerbate many existing medical conditions – so this semantic is not particularly helpful – and the GP and hospital clinical teams will already know this, as we also see this with seasonal flu.”
Prof James Naismith, Director of the Rosalind Franklin Institute, and Professor of Structural Biology, University of Oxford, said:
“The ONS data are incredibly useful as they give a true picture of the prevalence of the virus. Today’s release covering the period to the end of last week report the following:
(1) The prevalence England has followed the path of Scotland to reach 1 in 13 people with covid.
(2) The prevalence in Scotland most likely peaked at around 1 in 12 and should begin to drop.
(3) The prevalence in Wales has risen to 1 in 14, and Northern Ireland around 1 in 15 (the estimates for Wales and NI are more uncertain).
“Omicron BA.2 is extremely good at infecting people.
“It will be interesting to measure the percentage of the population that have been infected by BA.2, it appears from the data to have infected far more people than the other strains.
“It remains my view that unless you are completely shielded or are not susceptible to the virus, by the summer you are more likely to have been infected with BA.2 than not.
“No part of the UK has currently implemented effective control measures, the limit on prevalence of the virus is simply the proportion of susceptible people.
“This is literally living with the virus by being infected with it.
“Omicron BA.2 is less severe but the main reason we have endured this wave with many fewer deaths is vaccination. Vaccination has meant the elderly and vulnerable have been able to fight off this virus without very serious illness after being infected.
“Omicron BA.2 still kills the vulnerable unvaccinated.
“With such a high prevalence, as a country we have decided to run a long covid19 experiment. Long covid19 is recognised illness and there are now some clear markers for the disease.
“It seems likely with some evidence but not yet conclusively proven that vaccination significantly reduces the likelihood and severity of long covid, more work on long covid is urgently needed.
“The safety and efficacy of vaccines have been proven beyond any doubt.
“With such a high prevalence and long covid19 a clearly identified risk, I would urge everyone to get their first, second, third or fourth jag.
“I believe the data show that vaccination of children is very much a lower risk than the health problems faced by unvaccinated children who catch covid19.
“What is true here is true across the world, more effort to vaccinate our fellow humans in less developed countries is needed.”
Prof Kevin McConway, Emeritus Professor of Applied Statistics, The Open University, said:
“I had hoped, though not really expected, that this week’s release from the admirable ONS Coronavirus Infection Survey (CIS) might be a lot more encouraging than last week’s. But it isn’t. The latest estimates of positivity – the numbers who would test positive for the virus – are for the week 20-26 March. In that week, the total of the ONS estimates for the number of people who would test positive across the whole UK is about 4.9 million. Just a week earlier, it was about 4.3 million. That’s another really big increase – the best that I can find to say about it is that the increase isn’t as big as the increase of almost a million the week before. Of course, vaccination and the fact we have the Omicron variant now mean that the effect of all these infections won’t be anywhere near as serious as it would have been earlier in the pandemic. But people needing to take time off work or their caring responsibilities does seem to be reaching disruptive levels.
“The position does differ a bit between the UK countries, with ONS estimating that the trend in the latest week is increasing in England and in Wales, but saying that the trend is ‘uncertain’ in Scotland and in Northern Ireland. The proportion of people who would test positive varies between 1 in 12 and 1 in 15 across the four countries – a UK-wide figure allowing for the different populations of the countries is about 1 in 13. The estimated numbers testing positive for the most recent week is higher than it has been since the CIS began in England and in Wales, and those estimates go back to April 2020 in England and July 202 in Wales. In Scotland, the latest weekly estimate is the second highest it has ever been – the highest was for the previous week. The position in Northern Ireland is not so clear, partly because the statistical margins of error are wider there because fewer people are swabbed for the survey – it does look as if infections there may now be past their peak, but they have not fallen much from the peak yet.
“ONS estimate that the rate of testing positive increased again, in the most recent week, in all nine English regions, and the estimate is particularly high (1 in 11 testing positive) in the South West. In terms of age groups in England, ONS are saying that the rate of testing positive increased in all the age groups 25 years of age and older. In younger age groups, though rates have been increasing for the two weeks to 26 March, ONS consider that the trend is uncertain in the most recent week – maybe that’s a slight crumb of comfort that the increases in those groups may have slowed or even reversed, but we really can’t be sure of that yet. However, the rate of testing positive is still highest, of all the age groups, in the youngest group (age 2 years to school year 6), where ONS estimate that about 1 in 11 children would have tested positive on 23 March.
“How does this match up with what some people have been saying about the numbers of new confirmed cases on the Government dashboard, that there’s some sign of levelling off or even a small decrease? Well, I don’t think the dashboard figures provide very clear evidence of such a change in trend anyway, if one looks at the figures classified by the date people were tested rather than when their result was reported. More importantly, though, the dashboard cases can only give clear evidence of trends if there aren’t changes in who is being tested routinely, and of course there have been such changes and there will be more as free testing is wound down even more. That’s why we need the ONS survey more than ever.
“Arguably the closest match, in terms of trends, shouldn’t be between the CIS positivity estimates and the dashboard confirmed cases anyway. That’s because the positivity estimates include anyone who would test positive, whether their current infection has just begun or has been going on for days or weeks, while the dashboard figures for new cases are, well, just for new cases. The CIS also provides so-called ‘incidence’ estimates, which are for numbers of new infections. For technical reasons, however, the latest CIS incidence estimates are for about two weeks earlier than the latest CIS positivity estimates, and the statistical error bounds are relatively wider. This week’s latest CIS (modelled) incidence estimates go up to 16 March. For the week 10-16 March, the total CIS estimate of new infections is about 4.2 million, compared to about 3.1 million for the previous week. That’s about 600,000 new infections a day, not much less than 1% of the population. One in every hundred people being newly infected every day is a really high rate.
“I’ve commented for a few weeks now on the fact that the dashboard new case counts are falling much further behind the CIS incidence estimates that they used to be. The UK total of new confirmed cases on the dashboard for that week, 10-16 March, is only about 560,000 – in other words, routine testing was picking up only about 1 in every 8 of the new infections estimated by the CIS. You wouldn’t expect routine testing to pick up all of the infections, because some people don’t have any symptoms and some may choose not to be tested – but until about the start of February, generally a third and a half of the estimated new infections from the CIS were being recorded as new cases on the dashboard. So the fall to about an eighth is large, and not at all encouraging for the accuracy of dashboard trends in case rates.”
Prof Christina Pagel, Professor of Operational Research, UCL, said:
“Today’s numbers from ONS show incredibly high infection levels across the UK. England reached a record high for the most recent week, with high prevalence across all regions and age groups. Particularly concerning is the continued increase in the over 70s – over 7% estimated to be infected now compared to just under 2% at the height of the alpha wave in 2021. While vaccines (particularly boosters) are doing well, they are not perfect and we will see more deaths from Covid over the coming weeks, just as Scotland, whose BA.2 wave started a few weeks earlier than England, has seen a large 60% increase in Covid death certification this past week.
“While I suspect these we are at or close to peak now, I am worried that we could stay at these extremely high levels for several weeks yet (just as Northern Ireland has done this past month), with consequent disruption, sickness, more hospital admissions, deaths and long covid. I urge those who are eligible to get their 4th dose of vaccine and parents to take up the vaccine for 5-11 year olds before the next term. I will be continuing to wear my FFP2 mask in shops, public transport and face to face work meetings.”
Dr Stephen Griffin, Associate Professor in the School of Medicine, University of Leeds, said:
“The prevalence of SARS-CoV2 continues to astonish, and should not be ignored. The government “living with COVID” strategy of removing any mitigations, isolation, free testing and a considerable slice of our surveillance amounts to nothing more than ignoring this virus going forwards. Around half of the 20K or so COVID +ve patients in hospital at present are there directly because of the virus, and deaths are back to nearly 1000 per week.
“Aside from the acute toll upon human health, school disruption, and pressure on an already exhausted, understaffed and under-resourced NHS, such unchecked prevalence endangers the protection afforded by our vaccines and it is unclear how sustainable sequential emergency boosting programmes can be in response to this, and future variants. Our vaccines are excellent, but they are not silver bullets and ought not to be left to bear the brunt of COVID in isolation. Waning antibodies and the propensity of Omicron BA2 to re-infect people1 means further challenge to immunity from severe/symptomatic disease.
“Prevalence endangers the clinically vulnerable, who now will be less aware of community risks as a result of diminished testing; many have lived half-lives since the start of the pandemic. Prevalence increases the numbers of comparatively rare events, such as children becoming severely unwell. Prevalence challenges our waning vaccine immunity to infection, evidenced by older groups now showing more disease. Prevalence drives further increases in long COVID across all ages, as well as other complications that are being constantly uncovered, including recent revelations around diabetes, and, lastly, prevalence provides the means by which virus evolution continues en masse, eventually culminating in the next variant of concern.
“I urge the government to re-engage with public health, to safeguard our freedoms rather than to allow them at the public’s own risk, and to invest in the NHS and infrastructure challenges that will ultimately allow us to realistically live with, rather than endure this virus.”
1 https://www.biorxiv.org/content/10.1101/2022.03.30.486409v1
All our previous output on this subject can be seen at this weblink:
www.sciencemediacentre.org/tag/covid-19
Declared interests
Prof Kevin McConway: “I am a Trustee of the SMC and a member of its Advisory Committee. I am also a member of the Public Data Advisory Group, which provides expert advice to the Cabinet Office on aspects of public understanding of data during the pandemic. My quote above is in my capacity as an independent professional statistician.”
Dr Stephen Griffin: “Member of Independent SAGE.”
No others received.