

select search filters
briefings
roundups & rapid reactions
before the headlines
Fiona fox's blog
The Office for National Statistics (ONS) have released the latest data from their COVID-19 infection survey, looking at characteristics of people testing positive for COVID-19.
Prof Kevin McConway, Emeritus Professor of Applied Statistics, The Open University, said:
“This is the latest in a series of fortnightly bulletins from ONS, that give various information on characteristics of people who tested positive for SARS-CoV-2, the virus that causes Covid-19, in the Covid-19 Infection Survey (CIS). As always, these are people who were tested in the CIS because they were part of a representative sample from the community population of the UK. So they aren’t subject to the same sort of biases that can happen in data from routine testing, where changes in the numbers of people, and the types of people that are being tested, can make the results hard to interpret in terms of what’s really going on in terms of infections.
“This latest bulletin looks at two rather different aspects. First, it looks at how common it is to be reinfected, after a previous infection with the virus, and it aims to pick apart some characteristics of people who became reinfected. Some of that analysis is new, and hasn’t appeared before in such detail. Second, the bulletin looks at characteristics of the people who tested positive in a recent fortnight. This is the latest version of results that have appeared before in previous bulletins. Most of the findings on these characteristics are similar to what has been found before, so I will comment only very briefly on one aspect of that.
“The analysis of reinfections is, for me, certainly the more interesting part. ONS have looked at reinfection rates before, using data from the CIS and similar methods, but there’s more detail here. That’s largely because, when they have looked previously, there weren’t many reinfections, so statistically it was difficult to pick out characteristics that might affect the chance of being reinfected. Now the number of reinfections has increased, mainly because more time has passed, so the analysis can be more detailed. The methods that ONS and their collaborators use for these analyses are relatively new, and have developed over time – in appropriate ways, in my view. One aspect is that the definition of a reinfection has changed. In some previous work, a person could count as being reinfected if they had a positive test result 90 days after a previous positive test, with the most recent test result before the new positive results having been negative. (In the CIS, people are tested on more than one occasion, so such patterns of test results can be spotted.) More recently, the cut-off time has changed to 120 days, because in a few cases people could test positive, perhaps intermittently, for longer than 90 days. The new analysis covers reinfections between 2 July last year and 23 October this year.
“Possibly the most important finding is that reinfections are rare. That was already known from previous ONS bulletins, but this one reinforces it. The great majority of people who had tested positive in the CIS, and for whom enough time has passed so that they could count as a reinfection if they tested positive again, were not reinfected. Only 358 people were reinfected, out of almost 21,000 in the survey who could have been reinfected. ONS estimate that, if 100,000 people are at risk of reinfection, about 12 would be reinfected each day. That’s a low rate – it certainly does show that reinfection is possible, but it’s really not common. What’s more, many of those reinfections would involve quite a low viral load, so that (other things being equal) the person would be less likely to have severe illness. The rate of reinfection with a relatively high viral load (Ct less than 30 – the lower the Ct value, the higher the viral load is likely to be) in 100,000 people is about 6 a day, roughly half the figure for all reinfections.
“However, what is new this time is an analysis of factors that are associated with the risk of reinfection. I should say that, since this is observational data, if a factor is associated with the risk of reinfection, that doesn’t mean that that factor causes the increase risk. That’s because there will be many characteristics that differ between people who get reinfected and people who don’t, apart from the factors included in this analysis. The statistical model that is used for this analysis does adjust for each of the factors that were included, when estimating the association between each factor and the risk of reinfection, but those adjustments can’t allow for all the possible differences involved, so we can’t be certain about what causes what.
“That said, what results were found? Some are essentially already known from other work. The risk of reinfection was higher for people infected when Delta was the dominant virus strain, which fits in with the known fact that the Delta variant is more infectious. The chance of being reinfected is smaller in older people, though, on average, it goes down by only 9% (in a given period of time) with an extra ten years of age. In other words, suppose there were two groups of people, one aged 50 and the other aged 60, and they matched on the other characteristics included in the analysis. If 100 of those aged 50 were reinfected in a year, one would expect 91 of those aged 60 to be reinfected in a year. Since this result comes from a survey, there is statistical uncertainty – the data are consistent with the number of 60 year olds being reinfected being somewhere between 85 and 97, though a number near 91 would be more likely. It’s quite interesting that the risk falls with age rather than rising, but this analysis can’t tell us why.
“People who had symptoms when they were originally infected are less likely to be reinfected. A possible reason for that is that people who originally had symptoms may have had a stronger immune response the first time, which may have reduced their chance of reinfection later. This fits with another finding, that the lower the viral load (as measured by a higher Ct value) at the initial infection, the higher the chance of being reinfected. Again, that might be because those with a lower initial viral load may have had a weaker immune response, so are less protected against later reinfection. But this analysis can’t tell us directly that this is how it works in terms of cause and effect. The new analysis also found that people with a pre-existing long term health condition are more likely to be reinfected than people without such a condition.
“The analysis looked at several other possible factors that might have been associated with reinfection risk – sex, household size, working in patient facing healthcare, ethnicity, the level of deprivation where someone lives, and whether they had had two vaccinations. In each case the data are consistent with there being no association between the factor and the risk of reinfection. That doesn’t mean that there definitely is no association. That might be the case, but it could also be the case that there is an association but the data from the survey couldn’t establish that it exists. That might be particularly true for the factor of working in patient facing health care, because most people in the survey do not do that kind of work, so that the margin of statistical error for the comparison between patient facing health care workers and others is wide.
“It does looks surprising, at first, that the factor of having received a second vaccine dose is not associated with reinfection risk, in this analysis. One might expect the vaccination to reduce the risk. It’s possible that any such reduction is hidden in the results, because of associations between whether one had two doses and other factors included in the statistical model, such as age. “However, I think that it is most likely because what’s essentially going on is a comparison between double vaccinated people and everyone else. The ‘everyone else’ category would include unvaccinated people, but also people who had had one dose (which could possibly provide considerable protection against reinfection, given that a reinfected person has, by definition, previously had a natural infection). It’s also a possibility that some people’s initial infection occurred after they had been vaccinated – indeed for what’s probably a small number, they may have been vaccinated twice before their first infection, let alone their reinfection. So, really, I don’t think that we can read anything at all from these results about the effectiveness of vaccination against reinfection.
“The other analysis in this bulletin, of characteristics of people testing positive between 4 and 17 October, the great majority of whom would not have been reinfections, does show considerable reductions in the chance of being infected in people who have been vaccinated, compared to people who have not been vaccinated. Those figures can’t be used directly to estimate vaccine effectiveness against infection, because they don’t take account of all relevant factors, but they do give a pretty clear indication that vaccines make a pretty substantial reduction to the chance of being infected. So there’s decent evidence from this and other sources that vaccines are strongly associated with reductions in infection risk – but this bulletin doesn’t really tell us anything about any effect of vaccines on the risk of reinfection, as opposed to an initial infection.”
Prof Sheila Bird, Formerly Programme Leader, MRC Biostatistics Unit, University of Cambridge, said:
“Basic statistical reporting standards on re-infections could be better than in today’s report by ONS Community Infection Survey. Since “facts are chiels that winna ding”, the basics should include the numbers in bold that were not explicitly reported by ONS.
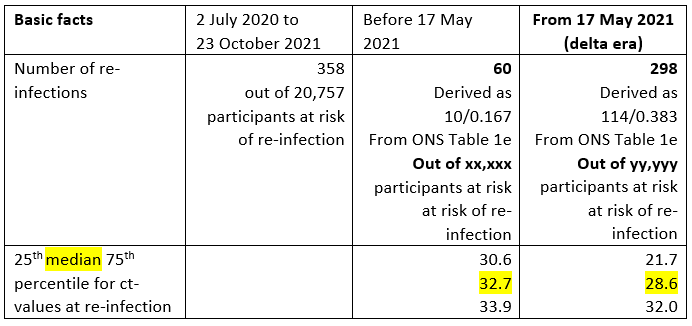
“Even allowing for vaccination and other risk-factors, ONS’s multifactorial Table 2a warns me that the risk of re-infection in the Delta era is higher by a factor of 1.7 (95% CI for hazard ratio: 1.26 to 2.40).
“Moreover, ct-values at re-infection in the delta era are dramatically lower (meaning higher viral loads) than before 17 May 2021.
“Face-validity for 1.7 is undermined because the basic facts provided by ONS do not include the number of participants at risk of re-infection in the Alpha versus Delta eras. Indeed, as Table 2a exemplifies, ONS typically fails to provide the basic descriptive data underlying its adjusted analyses – a reporting standard that medical journals would not accept.
“Hence, Table 2a does not tell us, for example, the number of non-white participants who were at-risk of re-infection, their number of person-years at risk and their number of re-infections. Nor does Table 2a report the number of participants at risk of re-infection in the delta era (yy,yyy in my Table), not their number of person-years at risk of re-infection in the delta era. I have derived that their number of re-infections was 298.
“The same failure to report basis data bedevils ONS’s Table 4a on risk factors for testing positive for SARS-CoV-2 infection during the most recent fortnight (4 to 17 October 2021). Hence, we do not know how many respondents had received “2 doses, AstraZeneca, more than 150 days ago”[A] and how many of them tested positive for SARS-CoV-2 versus the corresponding basic data for participants who had received “2 doses, Pfizer, more than 150 days ago” [P] and for the reference group of unvaccinated participants.
“Unadjusted for other covariates, the univariate impression will be a bit off-the-mark but readers like to have a sense of how far-off, and hence how much has been insight has been delivered by multivariable adjustment. ONS could do better.
“Fully-adjusted, [A] participants’ infection risk was reduced by 42% (95% CI: 26% to 55%) but [P] participants’ by 59% (95% CI: 47% to 68%) compared to the unvaccinated.”
Dr James Doidge, Senior Statistician, Intensive Care National Audit & Research Centre (ICNARC); and Honorary Associate Professor, London School of Hygiene and Tropical Medicine, said:
“The Coronavirus Infection Survey is one of the most valuable studies in the world right now, and this release provides further insight to the roles of prior infection and vaccination in generating immunity to COVID-19. The headline finding is that the rate of reinfection was 11.9 per 100,000 ‘person-days’, which equates to 1 in 23 people with prior infection for each year with infection rates comparable to those we have experienced since July 2020. However, a closer look at Figure 3 suggests that around one third of these supposed reinfections were in fact related to the original infection and not true reinfections (because the sharp rise at the start of the curve which represents approximately one third of supposed reinfections cannot be plausibly explained in any other way). While the authors did go to some effort to exclude original infections from their definition of reinfection, there appears to be substantial residual overcounting.
“This overcounting is important when considering the comparative benefits provided by prior infection versus vaccination in Figure 4. While the results indicate that prior infection provides somewhat better protection that nearly any level of vaccination (the only exception being having received a second dose of the Pfizer vaccine within the past three months), we should bare in mind that (1) about one third of those supposed reinfections experienced were not true reinfections, (2) that many of the people with vaccination will have also benefited from prior infection, and (3) that the vaccinations occurred on average much more recently than the prior infections. In short, prior infection clearly conveys considerably more protection than vaccination alone; but this is absolutely not to say that people who have not had confirmed prior infection should avoid vaccination in the hope of gaining protection via a natural infection instead. It does, however, raise serious questions about the net benefit of vaccinating people with known prior infection and about the ethics of vaccine mandates that do not allow for demonstration of the immunity provided by prior infection.”
All our previous output on this subject can be seen at this weblink:
www.sciencemediacentre.org/tag/covid-19
Declared interests
Prof Kevin McConway: “I am a Trustee of the SMC and a member of its Advisory Committee. I am also a member of the Public Data Advisory Group, which provides expert advice to the Cabinet Office on aspects of public understanding of data during the pandemic. My quote above is in my capacity as an independent professional statistician.”
Dr James Doidge: “None.”
None others received.